You can prevent a stroke to get to know and to control risk factors.
In the last 30 years, however, there has been a 45% reduction in deaths due to stroke. Today, 70% of people who suffer a stroke continue to have their independence, while 10% recover completely.
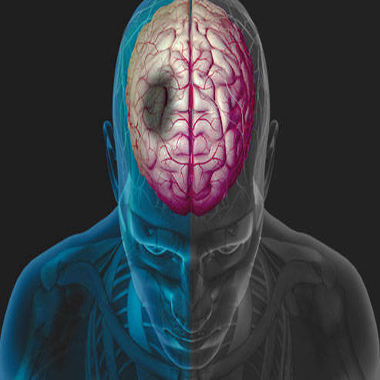
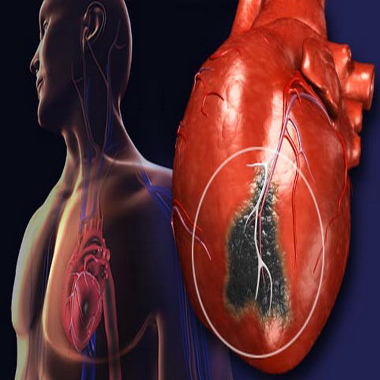
A stroke occurs when blood that flows to the brain through the arteries is disturbed or abruptly obstructed. Blood can stop flowing in an artery because it is obstructed by a blood clot or plaque (this is called ischemic stroke), or because the artery is broken or ruptured (this is called a hemorrhagic stroke).
There a numerous causes of stroke and they are usually associated with damage to the blood vessel walls, which slowly build up over time. Hypertension is a particularly common cause of vascular lesions.
Etiology
The causes are divided into congenital and acquired. Congenital causes primarily include vascular malformations (aneurysms, arteriovenous communications), congenital diseases of the heart, diseases of metabolism (e.g., homocystinuria) and of the blood (e.g., sickle cell anemia).
Acquired causes include:
- endocarditis,
- rheumatic fever,
- collagen diseases,
- hyperlipidemia,
- arteritis,
- thrombophlebitis,
- Heart valve diseases,
- diabetes mellitus,
- atherosclerosis,
- heart stroke,
- hypertension,
- coagulation disorders,
- amyloidosis,
- smoking,
- alcohol etc.
A patient suffering from one of the above conditions will not suffer a stroke. For this reason it is sound to refer to ‘risk factors for stroke”. Each factor alone increases the risk of stroke. If there is more than one factor, then the probability of the patient suffering stroke increases exponentially.
Pathogenesis
Each risk factor acts differently, but the result is always the interruption of the blood supply to a region of the CNS (ischemic stroke) or the rupture of a vessel with a subsequent hemorrhagic stroke.
The interruption of the blood supply may be caused by a clot which originates from the heart and travels through the great vessel to the brain (embolism). It may even be due to a thrombus from an adjacent vessel, or even in the same vessel (thrombosis).
In the majority of cases, the rupture of a vessel is due to lesions of the vessel wall resulting from chronic hypertension. It may even be due to vascular malformations in traumatic brain injuries, or other diseases of the walls
Clinical presentation
The clinical presentation of a stroke is dependent on the function of the area that was affected. Generally speaking, hemorrhagic strokes are considered to be more severe than ischemic strokes. This is because the blood that is diffuses the cerebral tissue causes relatively little damage (the blood is toxic for the brain tissue), it occupies space and places pressure on the brain. The brain is located in a rigid box as is the scalp and it is not able to shift to another space. Thus, any cause that places pressure on the brain can seriously harm it. Death may be instantaneous if pressure is applied to the brain stem (cases of herniation). If the bleeding is so small as not to apply pressure, then the patient’s prognosis is relatively good and he/she reaches full recovery.
The severity of an ischemic stroke depends on the size and importance of the vessel in which the blood flow was interrupted. Obstruction of the carotid causes hemiplegia, hemianesthisia, hemianopsia, total aphasia (left damage). Obstruction of the anterior cerebral artery may result death or disorders of consciousness, monoplegia primarily of the lower extremity, etc. Obstruction of the middle cerebral artery can cause hemiplegia, aphasia, sensory loss, hemianopsia, etc. Obstruction of the posterior cerebral artery can cause hemianopsia, thalamic pain, visual agnosia, etc.
Diagnosis
A stroke is clinically diagnosed and is based on the findings of a detailed neurological examination and the patient’s history.
Nevertheless, a computed axial tomography of the brain (Brain CT) is decisive given that many times it is difficult to clinically distinguish an ischemic stroke from a hemorrhagic stroke.
The patient should then undergo a complete diagnostic work up (blood tests, echocardiography and carotid U/S, etc.) to reveal the risk factors that caused the stroke.
Particular attention should be paid to cases where the symptoms completely subside only after a few hours. E.g. the patient feels a sudden weakness in one leg, but muscle strength returns to normal after a few hours. This patient most likely suffered a transient stroke. A transient stroke is defined as an episode in which symptoms subside within 24 hours. Mostly transient strokes last about one hour. It is possible that the reperfusion of the affected area is so fast that the damage is reversible, however, a large proportion of patients (approximately 20%) ischemic damage is revealed during CT. This is essentially a “small stroke”, therefore the patient should be treated as high-risk for a more serious stroke in the future.
How to recognize the signs of stroke or Transient Ischemic Stroke
To be able to recognize the signs of stroke, ask yourself three simple questions:
- Face – can the person laugh? Has his/her mouth or eye sagged/drooped?
- Hands – can the person raise both hands?
- Speech – can the person speak clearly and understand what you say?
- Time – act QUICKLY call 166
Stroke also includes signs of:
- Dizziness, loss of balance or unexplained fall
- Loss of vision, sudden or decreased vision in one or both eyes
- Headache is usually strong and occurs abruptly, or unexplained change in the form of headaches
- Difficulty in eating food or drinking liquids